Bacterial conjunctivitis, often called "pink eye", is a common eye infection caused by bacteria. It typically presents with symptoms like thick yellow discharge, redness, and eyelid sticking. While many cases clear up on their own, antibiotics can speed up recovery and reduce complications. Here’s a quick breakdown of treatment options:
- Fluoroquinolones (e.g., besifloxacin, moxifloxacin): Highly effective, especially for severe infections. Besifloxacin stands out for its broad bacterial coverage and low resistance rates.
- Polymyxin B/Trimethoprim (Polytrim): A solid choice for mild to moderate cases, especially in children. It’s effective against common bacteria but less so for MRSA.
- Ointments (e.g., erythromycin): Ideal for children and infants due to ease of application. Provides longer coverage but may cause temporary blurred vision.
- Observation: Mild cases often resolve naturally within 4–9 days. Supportive care like artificial tears and compresses can help.
- Systemic Antibiotics: Necessary for severe infections, such as those caused by Neisseria gonorrhoeae or Chlamydia trachomatis.
Each treatment has its pros and cons, and the choice depends on the severity of the infection, patient age, and specific needs. Severe symptoms like vision changes or significant pain require immediate medical attention.
WHAT CAUSES PINK EYE & HOW TO TREAT PINK EYE: youtube eye doctor explains conjunctivitis
sbb-itb-929a4e2
1. Fluoroquinolones (Ciprofloxacin, Moxifloxacin, Besifloxacin)
Fluoroquinolones are a go-to option for treating bacterial conjunctivitis due to their ability to target both gram-positive and gram-negative bacteria. This group includes older medications like ciprofloxacin and newer ones such as moxifloxacin and besifloxacin. However, bacterial resistance has become a growing issue. For instance, ciprofloxacin resistance among gram-positive bacteria rose from 11.7% to 35.6% over a decade. Resistance is particularly high in MRSA-related eye infections, with rates of 94% for ciprofloxacin and 68% for moxifloxacin.
Effectiveness
Besifloxacin has emerged as a standout option, with bacterial eradication rates surpassing 90% and clinical resolution rates reaching 70% or more by day five. In direct comparisons, besifloxacin achieved a 93.3% eradication rate, slightly higher than moxifloxacin’s 91.1%. Unlike other fluoroquinolones, besifloxacin was specifically developed for eye conditions, avoiding resistance linked to systemic treatments. It also demonstrates 8 to 128 times greater potency against ciprofloxacin-resistant MRSA and MRSE strains compared to other fluoroquinolones.
Patient Suitability
Choosing the right treatment depends on factors like the severity of the infection, patient age, and tolerance to the medication. Older fluoroquinolones, such as ciprofloxacin, are effective for less severe infections, while newer options like besifloxacin are better suited for more serious cases. Besifloxacin is approved for use in both children and adults, making it a flexible choice. For patients sensitive to preservatives, moxifloxacin (Vigamox) offers a preservative-free formula. Ciprofloxacin remains the best option against Pseudomonas aeruginosa, while levofloxacin is particularly effective against Streptococcus pneumoniae.
Application Method
Besifloxacin is typically applied as one drop three times daily for five days or twice daily for three days. It uses a mucoadhesive polymer called DuraSite, which extends the medication’s presence on the eye’s surface. This results in a mean residence time of 4.7 hours in the conjunctiva, compared to 3.0 hours for moxifloxacin. Older fluoroquinolones often require more intensive dosing, starting with applications every two hours for the first day or two, followed by four times daily.
Side Effects
Topical fluoroquinolones are generally well-tolerated, with fewer side effects than placebo (Risk Ratio 0.7). The most common issue with besifloxacin is mild conjunctival redness, affecting just 2% of users. Other minor side effects, such as blurred vision, eye pain, irritation, itching, and headaches, occur in only 1% to 2% of cases. Because these medications are applied directly to the eye, systemic absorption is minimal (less than 0.5 ng/mL), virtually eliminating the risk of systemic side effects. One exception is ciprofloxacin, which may occasionally leave white crystalline deposits in corneal ulcers, potentially causing confusion with infection.
2. Polymyxin B/Trimethoprim and Sulfacetamide
Polytrim (Polymyxin B/Trimethoprim) stands out with its dual-action approach to treating bacterial conjunctivitis. It combines Polymyxin B, which disrupts bacterial cell membranes, and Trimethoprim, which halts protein synthesis. This combination makes it effective against a variety of pathogens, including Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, and Pseudomonas aeruginosa.
Effectiveness
Clinical data reveals that about 95% of patients treated with Polytrim see improvement or complete resolution of symptoms within 7 days, with cure rates around 84% between days 2 and 7. While these results are comparable to other antibiotics like gentamicin and sulfacetamide, newer fluoroquinolones such as moxifloxacin may work faster. For instance, one study reported symptom resolution in 81% of patients within 48 hours using moxifloxacin, compared to 44% with Polytrim. Additionally, Polytrim matches the effectiveness of neomycin-polymyxin B-gramicidin (Neosporin) but tends to cause fewer side effects. These findings help clinicians decide when Polytrim is the right choice based on patient needs.
Patient Suitability
Polytrim is a great option for children aged 2 months and older, as it effectively treats common pediatric pathogens like Haemophilus influenzae. It’s also safe for breastfeeding mothers and elderly patients. However, it’s not suitable for severe infections like gonococcal or chlamydial conjunctivitis, which require systemic antibiotics. Its limited effectiveness against MRSA means alternative treatments like vancomycin may be necessary in those cases. Patients with allergies to any of its ingredients should avoid using this medication. When prescribed appropriately, Polytrim serves specific patient groups effectively.
Application Method
The recommended dosage is one drop in the affected eye(s) every 3 to 4 hours for 7 to 10 days. To prevent contamination, wash hands thoroughly before and after use and avoid touching the applicator tip to any surface. Contact lenses should not be worn during treatment or while symptoms persist. If your doctor approves resuming lens use, wait at least 15 minutes after applying the drops. The systemic absorption of the medication is minimal, with approximately 0.03 mcg/mL for trimethoprim and 1 unit/mL for polymyxin B.
Side Effects
Common side effects include local irritation such as redness, burning, stinging, and itching. Some patients may also experience eyelid swelling, tearing, rashes around the eyes, and intense itching. Less frequent side effects include blurred vision and increased sensitivity. In studies involving children, 62% of patients reported finding the treatment "very comfortable", while 27% rated it as "moderately comfortable". The drops should be stored at room temperature (59°–77°F) and protected from light. If symptoms don’t improve within 3 to 4 days, or if severe pain or vision loss occurs, seek medical attention promptly.
These attributes make Polytrim a strong contender when choosing a treatment plan for bacterial conjunctivitis.
3. Ointment-Based Treatments (Erythromycin, Bacitracin/Polymyxin B)
Ointment treatments like erythromycin and bacitracin/polymyxin B are a reliable option for bacterial conjunctivitis. Unlike drops, ointments stay on the eye longer, providing extended coverage against bacteria and making them a practical choice in treatment plans.
Effectiveness
Polymyxin B–bacitracin ointment shows a 62% clinical cure rate and 71% bacterial eradication within 3–5 days, compared to only 28% for placebo. Erythromycin achieves an impressive 96% clinical cure rate for neonatal chlamydial conjunctivitis. According to the American Academy of Ophthalmology, "No clinical evidence suggests superiority of any particular agent for mild cases".
Erythromycin and bacitracin target gram-positive bacteria, while combination ointments like polymyxin B/bacitracin expand coverage to gram-negative bacteria. Severe infections or contact lens wearers often require fluoroquinolone drops due to their stronger potency and ability to tackle pathogens like Pseudomonas. These efficacy rates help determine when ointments are the best option for different patient needs.
Patient Suitability
Ointments are particularly helpful for children since they resist being washed away by tears and are easier to apply. Erythromycin ointment (0.5%) is the go-to for preventing neonatal eye infections caused by N. gonorrhoeae or Chlamydia. Bacitracin works well for managing blepharitis when applied to the eyelid margins after cleaning away debris.
Erythromycin is often the most budget-friendly choice while still being effective. However, the temporary blurred vision caused by ointments – lasting around 20 minutes – may make them less practical for adults who need clear vision immediately. Contact lens users should avoid ointments during symptomatic periods, opting instead for fluoroquinolone drops.
Application Method
- Squeeze a 1/2-inch ribbon of ointment into the lower conjunctival sac.
- Tilt your head back, gently pull down the lower eyelid to create a pocket, and apply the ointment carefully without letting the tube tip touch your eye or skin.
- Close your eyes gently for 1–2 minutes to allow absorption.
- Use a clean tissue to wipe away any excess ointment from your eyelids or lashes.
| Medication | Common Strength | Typical Dosage | Primary Use |
|---|---|---|---|
| Erythromycin | 0.5% (5 mg/g) | 1 cm ribbon up to 6× daily | Mild cases, neonatal prophylaxis |
| Bacitracin | 500 U/g | 1 cm ribbon 1–3× daily | Gram-positive infections, blepharitis |
| Polymyxin B/Bacitracin | 10,000 U / 500 U/g | Apply every 3–4 hours | Broad-spectrum coverage |
Always wash your hands before and after applying the ointment. Continue treatment for 5–7 days or until symptoms resolve, but complete the full course to reduce the risk of recurrence or antibiotic resistance. Watch for any side effects during treatment.
Side Effects
The most common side effect is temporary blurred vision. Other possible reactions include burning, redness, itching, swelling, or slower healing. Serious symptoms, such as intense pain, worsening discharge, rash, hives, or breathing difficulty, require immediate medical attention. If symptoms don’t improve within 3–4 days, consult your eye care provider.
Store ointments at room temperature (59°–77°F) and away from direct light or heat. Never freeze them. To avoid spreading infection, don’t share eye products, towels, or washcloths.
4. Observation and Systemic Antibiotics
Mild bacterial conjunctivitis often clears up on its own without the need for medication. The American Academy of Ophthalmology advises against routine antibiotic use for acute conjunctivitis because most cases resolve naturally. However, severe infections – such as those caused by Neisseria gonorrhoeae or Chlamydia trachomatis – require immediate systemic antibiotics to prevent complications. Treatment decisions hinge on the severity of the infection.
Effectiveness
For uncomplicated cases, around 55% of patients recover within 4–9 days without antibiotics. Using topical antibiotics can increase recovery rates to 68.2%. The Centers for Disease Control and Prevention (CDC) notes that mild bacterial conjunctivitis typically clears up in 2 to 5 days without treatment, although full recovery may take up to two weeks.
In high-risk situations, systemic antibiotics are crucial to avoiding severe complications like corneal perforation or meningitis. For instance, gonococcal conjunctivitis is treated with a single intramuscular dose of ceftriaxone (1 g) along with a 1 g oral dose of azithromycin. Chlamydial conjunctivitis is addressed with either a single 1 g dose of azithromycin or a course of doxycycline.
Patient Suitability
Observation is a practical approach for adults and children with mild symptoms, such as slight redness and minimal discharge, as long as there are no changes in vision or severe pain. Supportive care – like cold or warm compresses and preservative-free artificial tears applied 2 to 6 times daily – can help relieve discomfort. On the other hand, systemic antibiotics are necessary for specific groups, including:
- Newborns showing any signs of conjunctivitis.
- Sexually active adults suspected of having gonococcal or chlamydial infections.
- Patients with conjunctivitis-otitis syndrome.
Immediate medical attention is vital if symptoms like severe eye pain, extreme sensitivity to light, or persistent blurred vision occur.
Side Effects
Observation avoids the risks associated with medication but carries a small chance of complications like keratitis or orbital cellulitis. Rarely, primary meningococcal conjunctivitis may lead to meningitis in about 18% of cases, and roughly 25% of children with Haemophilus influenzae conjunctivitis may develop otitis media.
Systemic antibiotics, while effective for severe infections, expose patients to significantly higher drug levels – up to 10 million times more than topical treatments. This can increase the risk of antibiotic resistance and side effects, including gastrointestinal issues, headaches, and, in rare cases, allergic reactions. Despite these risks, systemic antibiotics remain indispensable for managing serious infections.
Next, we’ll weigh the pros and cons of these treatment approaches.
Comparing Treatment Benefits and Drawbacks
Bacterial Conjunctivitis Treatment Options Comparison Chart
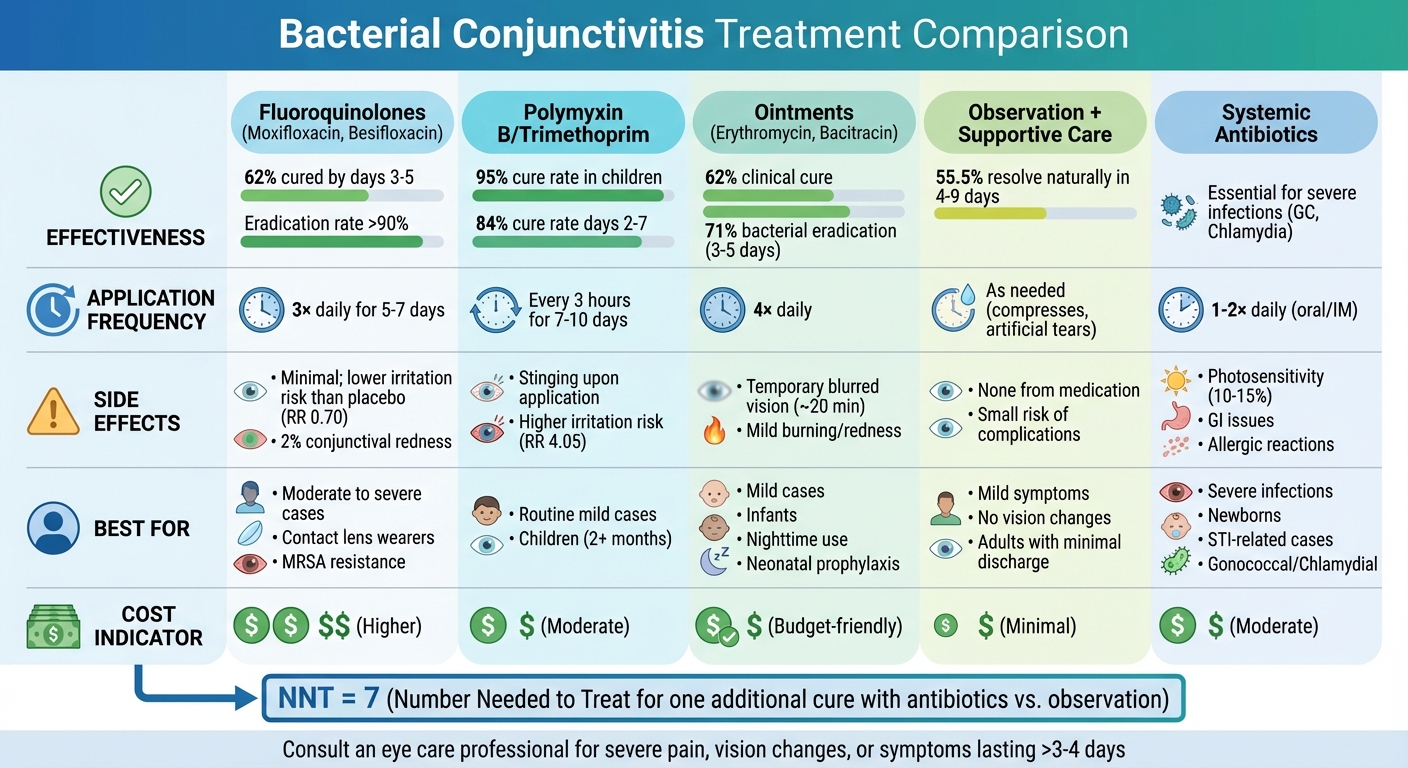
Choosing the right treatment for bacterial conjunctivitis involves weighing factors like effectiveness, dosing schedules, side effects, and cost. Research shows that all antibiotic classes achieve similar clinical cure rates, with no major difference between fluoroquinolones and older antibiotics in clearing infections. However, practical considerations vary, and these differences can influence treatment decisions.
Fluoroquinolones, such as moxifloxacin and besifloxacin, are more convenient with just three applications per day, compared to polymyxin B/trimethoprim, which requires dosing every three hours. While fluoroquinolones are typically more expensive, they are associated with a lower risk of irritation (RR 0.70) compared to non-fluoroquinolones, which have a higher irritation risk (RR 4.05). For non-fluoroquinolone antibiotics, the Number Needed to Treat (NNT) for avoiding adverse effects is 32.
Ointment-based treatments, like erythromycin, stay on the eye longer, making them helpful for overnight relief. However, they can cause temporary blurred vision, which limits their use to children or bedtime for adults. Additionally, about 10% of patients are allergic to ingredients like neomycin or bacitracin found in triple-antibiotic ointments, so checking for allergies is critical.
Interestingly, mild cases of bacterial conjunctivitis often resolve on their own. About 55.5% clear up naturally within 4–9 days. Adding antibiotics can increase cure rates to 68.2%, but the NNT is 7, meaning seven patients need treatment for one additional cure. According to the American Academy of Family Physicians:
Topical antibiotics may speed up clinical and microbiological cure of bacterial conjunctivitis, but the benefit is small.
The table below summarizes the effectiveness, dosing schedules, side effects, and ideal use cases for different treatment options:
| Treatment Category | Effectiveness | Application Frequency | Common Side Effects | Best For |
|---|---|---|---|---|
| Fluoroquinolones (Moxifloxacin, Besifloxacin) | High; 62% cured by days 3–5 | 3x daily for 7 days | Minimal; lower irritation risk than placebo | Moderate to severe cases; contact lens wearers |
| Polymyxin B/Trimethoprim | High; 95% cure rate in children | Every 3 hours for 7–10 days | Stinging upon application; higher irritation risk | Routine mild cases; children |
| Ointments (Erythromycin, Bacitracin) | Standard; effective for common pathogens | 4x daily | Temporary blurred vision | Mild cases; infants; nighttime use |
| Observation + Supportive Care | 55.5% resolve naturally in 4–9 days | As needed (compresses, artificial tears) | None from medication | Mild symptoms; no vision changes |
| Systemic Antibiotics | Essential for severe infections (GC, Chlamydia) | 1–2x daily (oral/IM) | Photosensitivity (10–15%) | Severe infections; newborns; STI-related cases |
When to Seek Care at Denver Eye Surgeons
While most cases of bacterial conjunctivitis clear up without antibiotics, there are times when symptoms demand immediate attention. If you experience moderate to severe eye pain, blurred or decreased vision, or intense sensitivity to light (photophobia), it’s crucial to seek care promptly. These symptoms could signal a condition that, if left untreated, might jeopardize your vision.
Some situations call for even more urgent action. For example, if you notice heavy discharge, significant eyelid swelling, or rapidly worsening redness, you should contact an eye specialist within 24 to 48 hours. Certain infections, like those caused by Neisseria gonorrhoeae, can progress quickly and may lead to severe complications, such as corneal perforation, without prompt treatment. Other warning signs, like flashes of light, dark spots in your vision, or a foreign body sensation, also warrant an urgent evaluation.
For contact lens wearers, it’s especially important to stop wearing lenses at the first sign of redness or irritation. This group faces a higher risk of bacterial keratitis, which affects 10 to 30 out of every 100,000 wearers annually. Lenses should not be used again until all symptoms have fully resolved. Additionally, newborns showing any signs of pink eye require immediate medical attention to prevent complications like blindness or systemic infections.
If your symptoms don’t improve after 2 to 3 days of treatment or persist for more than 4 weeks, it’s time to consult a professional. Persistent symptoms, despite initial treatment, may indicate a more complex issue requiring specialized care. Acting quickly in these cases ensures a more effective resolution.
Denver Eye Surgeons is well-equipped to handle such cases, offering over 40 years of expertise and access to advanced diagnostic tools. Their team specializes in managing difficult eye conditions, including chronic or severe conjunctivitis. As they explain:
Our doctors at Denver Eye Surgeons see pink eye regularly and they are very experienced in making the correct diagnosis and recommending the appropriate treatment.
For persistent or unusual cases, they use advanced techniques like conjunctival scrapings and bacterial cultures to identify the root cause and guide treatment.
While waiting for your appointment, take precautions to prevent spreading the infection. Wash your hands frequently, and avoid sharing items like towels, makeup, or eye drops. Denver Eye Surgeons also offers same-day appointments for urgent cases, ensuring you get the care you need without unnecessary delays.
Conclusion
Treating bacterial conjunctivitis effectively depends on the severity of the infection. Comparing older antibiotics, newer fluoroquinolones, and systemic treatments shows that the right choice varies based on the patient’s needs. For mild cases, older antibiotics like trimethoprim/polymyxin B often work well. Moderate to severe infections, however, may require newer fluoroquinolones. In extreme cases involving pathogens like N. gonorrhoeae or Chlamydia, systemic antibiotics are essential to prevent serious complications.
Getting the diagnosis right is just as important as the treatment itself. Proper evaluation helps differentiate bacterial conjunctivitis from other conditions like viral or allergic conjunctivitis, or even more serious issues such as acute glaucoma or keratitis. This ensures the patient receives the right treatment without unnecessary use of antibiotics.
"The mainstay of treatment for bacterial conjunctivitis is topical antibiotic therapy, with the intent of significantly reducing the duration of symptoms and likelihood of contagion." – Karen K Yeung, OD, FAAO
Timely diagnosis and appropriate treatment lead to quicker recovery and better outcomes. Early medical attention can reduce the duration of symptoms, limit the spread of infection, and prevent complications like corneal scarring or perforation. For individuals with severe symptoms, such as vision changes or intense pain, or for groups like contact lens wearers and newborns, immediate professional care is especially critical.
If you’re dealing with symptoms of bacterial conjunctivitis or have concerns about your eye health, it’s important to act quickly. Denver Eye Surgeons provides same-day appointments and brings over 40 years of experience in treating various eye conditions. Their team uses advanced diagnostic tools to ensure you get the right care for your specific condition, helping you recover safely and efficiently.
FAQs
How can I tell bacterial pink eye from viral or allergic conjunctivitis?
Bacterial conjunctivitis often leads to a thick, pus-like discharge that can cause the eyelids to stick together, particularly after sleeping. It usually begins in one eye but can spread to the other. Viral conjunctivitis, on the other hand, is characterized by watery discharge and is often associated with cold-like symptoms. It typically affects one eye first, then the other. Allergic conjunctivitis stands out with intense itching, redness, and watery discharge, frequently accompanied by allergy-related issues like sneezing or a stuffy nose.
Do I really need antibiotic drops, or can I wait it out?
Bacterial conjunctivitis typically resolves on its own within 2–5 days, so simply waiting it out can be an option. That said, antibiotics can help speed up recovery and minimize the chances of passing it to others. If symptoms linger beyond 1–2 days, starting treatment is usually advised to promote quicker relief and limit the risk of spreading the infection.
When should I seek urgent care for pink eye symptoms?
If your pink eye is accompanied by severe pain, changes in vision, intense redness, or if your symptoms worsen or fail to improve within a few days, it’s crucial to seek urgent care. These could be warning signs of a more serious issue requiring immediate medical attention.